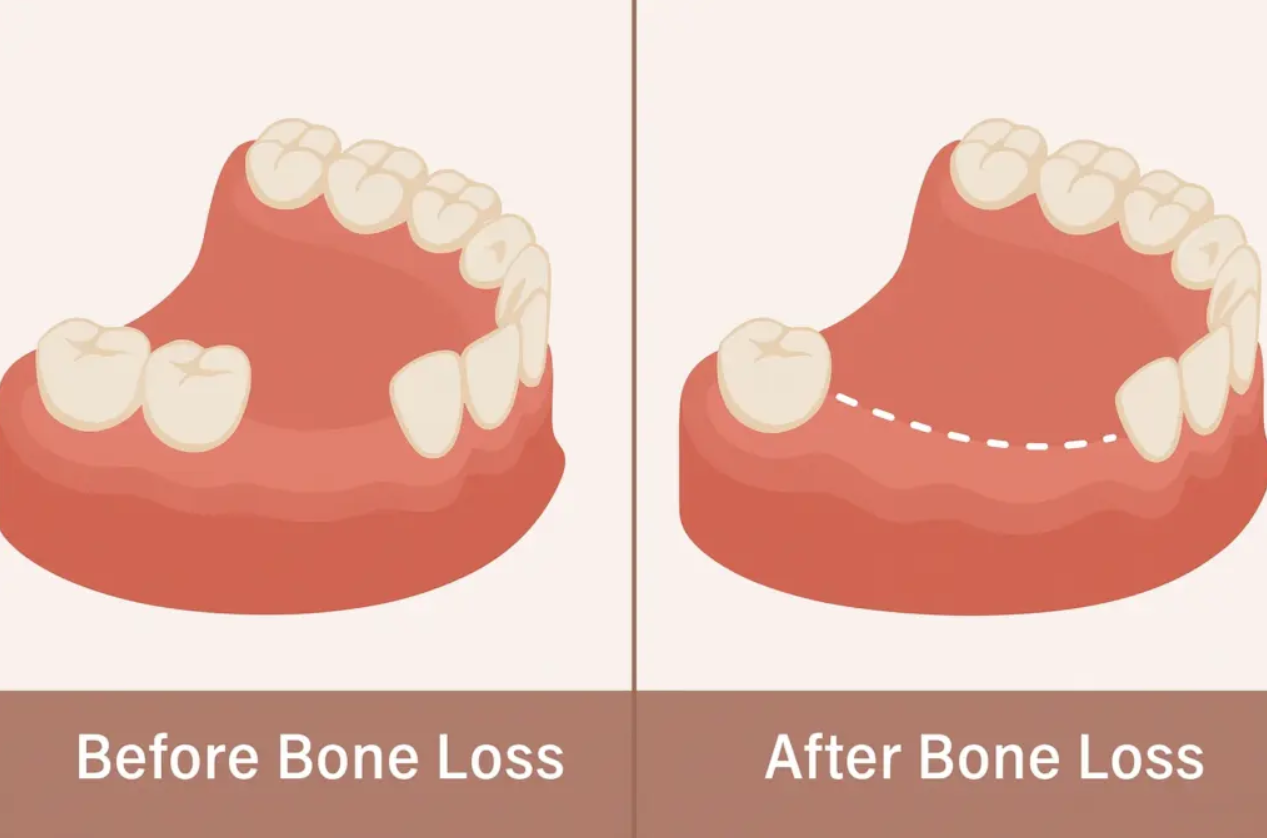
You can lose jawbone even if you have all your teeth. The bone shrinks when support and repair fall out of balance from disease, missing teeth, systemic health issues, or trauma.
If infection, untreated gum disease, or long-term mechanical changes weaken the bone faster than your body rebuilds it, your jaw can deteriorate without obvious tooth loss. This can happen quietly, so it’s easy to miss until there’s a bigger problem.
You’ll find out how biology (like osteoporosis and inflammation), local dental conditions (gum pockets, infections, tooth loss nearby), and lifestyle factors (smoking, poor hygiene, diet) all play a role in bone loss. Practical steps for prevention and long-term management follow, so you can protect your facial structure and keep your smile stable—and if bone loss has already progressed to the point of tooth loss, dental implant surgery in Las Vegas offers a proven way to restore both function and jaw health at the same time.
Biological Factors Influencing Bone Health
Several internal processes determine how quickly you lose bone and how well your skeleton repairs itself. Hormone levels, inherited genes, and chronic diseases can all speed up bone loss or slow down repair.
Aging and Hormonal Changes
As you age, bone remodeling shifts. Cells that break down bone (osteoclasts) start to outpace cells that build bone (osteoblasts).
After age 50, both men and women experience net bone loss. Women lose bone faster during the decade after menopause because estrogen—a hormone that limits osteoclast activity—drops sharply.
Low estrogen increases bone turnover and reduces mineral density, raising fracture risk even if you still have teeth. In men, gradual declines in testosterone and sometimes low estrogen from aromatization lead to slower but still significant bone loss.
Age also reduces calcium absorption and vitamin D activation in the kidneys. That only makes things worse.
Genetics and Family History
Your peak bone mass and lifelong bone-loss trajectory depend a lot on heredity. Variants in genes controlling collagen structure, vitamin D receptors, and the regulators of bone-building and bone-breaking cells explain why bone density differs so much between people.
If a parent had osteoporosis or a hip fracture, your fracture risk goes up—even if your own bone density looks okay. Family history can also signal inherited endocrine or connective-tissue disorders, like osteogenesis imperfecta or familial hypophosphatasia, that directly weaken bone.
Genetic risk should shape how often you get screened and how aggressive you are with prevention.
Systemic Diseases Affecting Bone Density
Some chronic conditions speed up bone loss by changing hormones, nutrient absorption, or inflammation. Hyperthyroidism increases bone turnover and reduces density.
Primary hyperparathyroidism causes calcium to leach from bone. Long-standing inflammatory diseases—like rheumatoid arthritis or inflammatory bowel disease—raise cytokines (IL-1, IL-6, TNF) that stimulate osteoclasts.
Metabolic conditions like chronic kidney disease impair vitamin D activation and phosphate handling, weakening bone mineralization. Malabsorption from celiac disease or gastric bypass limits calcium and vitamin D uptake.
Prolonged glucocorticoid therapy suppresses bone-building cells and accelerates bone breakdown, sometimes within months of starting treatment.
Local Conditions That Lead to Deterioration
Local oral problems can directly reduce the bone that supports your teeth. Inflammation, force changes, or infection and injury can all destroy bone tissue.
Chronic Gum Inflammation
When your gums stay inflamed, your body breaks down the fibers and bone that hold teeth in place. Plaque bacteria trigger an immune response that releases enzymes and cytokines.
Over weeks to years, that immune reaction erodes the alveolar bone around tooth roots. Bleeding, gum recession, or pockets forming between teeth and gums are warning signs that bone loss is happening.
Controlling inflammation with better home care, professional cleanings, and targeted periodontal therapy helps reduce the chemical signals that cause bone resorption. In moderate to advanced cases, your dentist may suggest scaling and root planing, localized antibiotics, or even periodontal surgery to stop progression and try to regenerate lost bone.
Tooth Misalignment and Bite Issues
Misaligned teeth or an uneven bite put extra chewing forces on specific teeth and the underlying bone. Chronic pressure causes bone resorption at overloaded sites, while other areas don’t get enough stimulation to stay healthy.
You might notice tooth mobility, uneven wear patterns, or jaw muscle tenderness. Orthodontic correction, bite adjustments, or night guards can redistribute forces and protect bone.
Fixing malocclusion early helps prevent the slow bone loss that comes from years of uneven mechanical stress.
Jawbone Trauma or Injury
Blows to the jaw—accidents, sports injuries, or repeated hits—can fracture bone or damage the blood supply that keeps bone healthy. If circulation gets compromised or infection sets in after an injury, bone breaks down faster around those teeth.
Even blunt force that just bruises the bone can cause microscopic damage that weakens support over time. Quick evaluation, proper fracture management, and infection control matter a lot.
If you lose bone, surgical options like bone grafting or guided bone regeneration can help restore structure to support teeth and future dental work.
Lifestyle and Environmental Contributors
Everyday choices and exposures can weaken the bone that supports your teeth. These factors change bone remodeling, reduce mineral supply, or increase inflammation, raising your risk of jawbone loss even if your teeth seem fine.
Dietary Deficiencies
Not getting enough calcium and vitamin D means your body lacks the raw materials to maintain alveolar bone. If your diet skips dairy, fortified plant milk, leafy greens, or fatty fish, your bones might not get enough calcium.
Low sun exposure or poor dietary vitamin D lowers calcium absorption. Protein matters, too—very low protein intake slows bone repair, and poor nutrition in general means slower healing after gum injury or infection.
Micronutrients like vitamin K2, magnesium, and phosphorus also support bone mineralization. Restrictive diets (very low-calorie, elimination diets) without supplementation or monitoring can increase your risk.
If you have signs of bone loss or dietary restrictions, ask your clinician for a vitamin D test and basic bloodwork. Consider targeted dietary changes or supplements based on the results.
Medication Side Effects
Some common medications mess with bone turnover or oral health. Long-term corticosteroids (oral or high-dose inhaled) reduce bone formation and increase resorption, raising the chance of alveolar bone loss.
Antiresorptive drugs like bisphosphonates and denosumab reduce bone turnover and protect systemic bone, but they carry rare risks for jaw complications. Always talk to your prescriber before dental procedures.
Antidepressants (SSRIs) and certain anticonvulsants can lower bone density if you use them long-term. Proton pump inhibitors, if taken for a long time, impair calcium absorption by reducing stomach acid.
Tell your dentist about these medications before extractions or implants. Schedule more frequent periodontal monitoring to catch early bone changes.
Smoking and Alcohol Consumption
Smoking reduces blood flow to gum and bone tissue and weakens the immune response. That makes it harder to control the infections that drive bone loss.
Nicotine and tobacco smoke disrupt fibroblast function and slow wound healing after dental treatment. Quitting smoking really does lower your risk of continued bone loss and improves outcomes after periodontal therapy.
Heavy drinking messes with calcium balance, hormone regulation, and liver function, all of which can reduce bone formation. Binge or chronic drinking can also worsen oral hygiene and increase your risk of periodontitis.
If you smoke or drink heavily, ask your healthcare team for help quitting. You’ll probably need a tailored oral health plan with more frequent cleanings and bone checks.
Prevention and Long-Term Management
You can slow or prevent dental bone loss by combining regular professional care with targeted nutrition and lifestyle steps. Focus on consistent checkups, infection control, and daily habits that support bone density and gum health.
Routine Dental Assessments
Schedule dental checkups every 3–6 months if you have gum disease risk factors like smoking, diabetes, or a history of periodontal disease. Otherwise, plan at least one visit every six months.
At your visits, your dentist or hygienist should measure pocket depths, check for gum recession, and take periodic X-rays to monitor bone levels.
Follow professional recommendations for scaling and root planing when pockets exceed 4 mm. Get maintenance cleanings more often if inflammation sticks around.
If you have implants or restorations, ask for targeted checks of the surrounding bone and soft tissue. Keep your X-rays on file so your dental team can compare bone changes over time and adjust your treatment early if needed.
Nutritional Strategies for Bone Strength
Aim for a daily calcium intake of about 1,000–1,200 mg. Get most of it from food—dairy, fortified plant milks, canned salmon with bones, and leafy greens all work well.
Pair calcium with enough vitamin D. Shoot for 600–800 IU each day, ideally from sunlight, but supplements can help if your blood levels are low.
You might want to ask your provider for a 25(OH)D test to figure out your vitamin D needs. It’s worth checking since everyone’s different.
Include some protein at every meal to help your bones and support tissue healing. It doesn’t have to be fancy—beans, eggs, yogurt, or a handful of nuts will do.
Try to limit alcohol, and honestly, it’s best to skip smoking altogether. Both can speed up bone loss more than you’d expect.
If you like checklists, keep it simple: eat calcium-rich foods, check your vitamin D, move your body with weight-bearing activities, and keep sodium and soft drinks in check. That combo goes a long way for bone health.



